By Dr Raghuram Y.S. MD (Ay).
We all have lost our tail with evolution…but did you ever think that the vestigial (redundant) part of that tail which has been left over in us in the form of tailbone can mess up with our daily activities and torture us to the level of not allowing us to sit!
If you are not able to sit or if you are experiencing pain when sitting right at the tail bone region, you may be having ‘Tailbone Pain or Coccydynia’.
Table of Contents
What is Coccydynia?
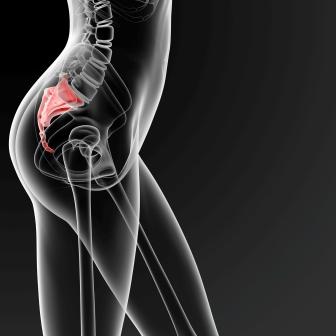
It means coccyx bone pain or tailbone pain. Coccyx is a bony area located between the buttocks and the anus.
Along with pain, it is also associated with tenderness at the tip of the tailbone and can be experienced between the buttocks
It occurs due to the inflammation of the tailbone. It is also defined as a type of back pain felt at the base of the spine. The pain is usually brought on by sitting too abruptly or often worsened by sitting.

Clinical features
- Pain in the coccygeal region (tip of the tail bone)
- Local tenderness
- The pain can range from mild to severe. It is usually worse when
- Sitting down
- Moving from sitting to a standing position
- When touched or when some pressure falls on the coccyx
- Worsens with constipation, feels better after bowel movement
- Some people can tolerate sitting in the same position for only a few minutes. They feel restless after a few minutes. They have to get up and move around to get relieved of the pain
- Pain makes everyday activities difficult Ex. Driving, bending over, sitting down etc.
- Sitting on a soft surface may be more painful than sitting on something hard. Sitting on a soft surface places most of your weight on your coccyx rather than on the hard bones below your pelvis.
- Difficulty in sitting and leaning against the buttocks
Other symptoms:
- Backache
- Shooting pain down to the legs
- Pain before or during defecation
- Pain during sex (aggravates at or after sex)
- Painful buttocks and hips
- Increased pain during monthly periods in women
- Difficulty to sleep comfortably at night, you may need to keep changing the positions while your sleeping.
- Symptoms usually improve with relief of pressure when standing or walking
Tips to relieve coccyx pain
Do not sit leaning backward. Coccydynia pain occurs more while the person sits leaning backwards. Hence, try to sit straight or slightly leaning forward, while keeping the lower back straight.
Do not sit for long hours. Consider moving around once in 30 – 45 minutes.
Obesity: If you are over-weight, while sitting, the coccyx has to bear that much extra weight. Hence, follow these obesity tips and lose weight.
Cold and hot packs: If you are diagnosed with coccydynia, and are experiencing pain, then for the initial 2 – 3 days, keep an ice pack over the painful area for 10 minutes twice a day. This would reduce the pain. After the third day, for the next one week, keep warm water pack for 10 minutes twice a day. Before giving hot water pack, apply Mahanarayana oil over the painful area. This would help in bringing down inflammation.
Do not carry excessive weight. This reduces the pain and pressure on coccyx bone.
Sitting: Specially designed gel-filled cushions can reduce pain when you are sitting. It also helps you to lean forward and rest your arms in front of you on a flat surface such as that of a table. This takes the pressure off your coccyx.
Avoid sitting for a long period of time whenever possible.
Sitting on a pillow, cushion or a buttock support. Use a well-padded seat when sitting
Clothing: Clothing like tight jeans or trousers may worsen your coccydynia. Wear loose-fitting clothes that will not put pressure on your coccyx. Also wear flat comfortable shoes

Sleeping: With coccydynia, sleeping on the sides will be uncomfortable. If you have severe pain, sleep on your front to feel better. Try sleeping with pillow or cushion between your knees.
Swimming for at least 20 minutes a day with 5 minutes of kicking warm up will better the pain of coccydynia (though it may not help to completely get rid of the pain)
Exercises for coccydynia
The below said exercises relieve stress of the muscles around the coccyx after sitting for a long time. This release the tension built up around the muscles in the coccyx.

Kneeling groin stretch:
A kneeling groin stretch can help prevent coccyx pain from occurring after long periods of sitting (Adductor Magnus is a muscle which contributes to tailbone pain when it is tight. It gets stretched during this exercise and helps prevent tailbone pain.)

Hands to feet stretch
Stand straight. Start bending down while keeping the legs straight (do not bend it at knee). Try to touch your feet. Hold the position for 10 seconds. Stand straight. Repeat this, five times a session, two sessions per day. Increase it to 10 times a session after a week time.
Piriformis stretch
Lie on your back.
Cross your left leg over your right so that your ankle rests on your right knee.
Use your hands to grab hold of your left knee and pull it gently toward the opposite shoulder
Hold for 15 to 30 seconds
Relax, and then repeat with the other leg
Repeat this cycle 2 to 4 times
read related
Walking:

- Walking should be done at least for 15 – 30 minutes at brisk pace.
- Normally the coccyx gets stuck in a wrong position. Then it provokes a muscle spasm. The spasm then blocks the coccyx which gets stuck by the muscles. This gets worse with passage of time. Sometimes it may lead to nerve entrapment in the coccygeal area.
- It is necessary to unblock the coccyx and relax the muscles as soon as possible. The best option to achieve it is to walk fast for many hours a day.
- Walking has a powerful relaxing effect on the spasms that tends to build up around coccyx
- Strolling just doesn’t work
Caution: The coccyx position can give you pain sometimes even as you walk for a short distance. In such case you should gradually build up your walk by taking short breaks in between.
Exercises videos
Exercises for Tailbone pain (coccydynia) – Videos:
https://www.youtube.com/watch?v=UqP77GD6JAo
Leg Exercises:
The leg exercises definitely will help you to get rid of coccyx pain. Try the exercises as explained in the video.
https://www.youtube.com/watch?v=SYJy_bsCJqo
Anal lock (Mulabandha):
Anal lock or pelvic lock exercise reduces sacral pain and coccyx pain. This exercise is usually done in the bed both in the morning and evening.
https://www.youtube.com/watch?v=qgHt9y0RPGg
We have already done it million of times. Whenever we have an urge to defecate we hold on by tightening some muscles in our anal region so that we don’t get it there right away. Anal lock involves the same muscles.
Rhythmically contracting, holding then releasing these muscles –
- Stimulates nerves and local blood flow
- Tones and strengthens your pelvic muscle and
- Relieves pain in the sacrum and coccyx
This is a simple exercise and can be done while standing, sitting or lying down.
Caution: if you have a history of problems in the lower back, sacral or coccyx region check with your doctor before trying this exercise.
How to do?
Holding the contraction:
- Gently contract your anal sphincter muscles
- Hold the contraction as tightly as you can without causing discomfort (for 10-12 seconds)
- Feel the contraction in your sacral, pelvic and abdominal area as you hold the contraction
- Initially you will not feel tightness in all these areas. You will appreciate this with practice and greater muscle control over a period of time.
Releasing the contraction:
- Now gently release the contraction
- Take a slow, deep breath and exhale
This completes 1 round
To begin with try doing 3-5 rounds
Build up 10-15 rounds or simply do the exercise a couple of minutes, several times in a day
Benefits:
- Stimulates nerves in the sacral and coccyx region
- Tones and strengthens the pelvic area
- Eases the pain in the sacrum and coccyx
Note: Do this exercise in bed before you get up and again at night
The anal lock can assist in the medical treatment of:
- Pain in the sacrum area including the sacral joints
- Lumbar sacral strain and injuries
- Sacral iliac pain
- Coccyx injuries, pain and bruises
Clam shell exercise:
Videos for clamshell exercise:
https://www.youtube.com/watch?v=7iXpLxKs1sY
How to do?
- Start in the side-lying position with knees bent
- From this position, raise your knee using your gluteal medius at the side of your hips
- Hold the top position for 5 seconds
- Work out for up to 10 second holds and repeat for 10 times
Yoga for coccydynia
Ardha Shalabhasana (The Half-Locust posture)
Video for Ardha Shalabhasana:
How to do?
- Lie on your stomach with the chin stretched and touching the ground
- Keep the hands on the side
- Slowly bring your hands under the legs to support them
- Inhale slowly and deeply and lift your right leg upwards, without bending the knees, as much as you can and without straining
- Maintain this position for few seconds, maximum up to ½ minute
- Slowly release the position by bringing down the right leg back to the original position
- Exhale during this process
- Rest for few seconds and breathe normally and deeply
- Next try the above steps with your left leg lifted above the ground
- This process can be done a few times alternating between the right and left leg
Shalabhasana (Full Locust pose posture):
Video for Shalabhasana:
https://www.youtube.com/watch?v=IKDTZmKm_g0
How to do?
- It is similar to Ardha Shalabhasana but you should lift both the legs together instead of one at a time
- Maintain this position for a few seconds to maximum of half a minute, without straining
- Bring both legs back to the starting position
- After the asana, one can rest by putting the arms below the head like a pillow and resting the head on one side. Breathe normally and deeply in the resting position
Benefits of Shalabhasana and Ardha Shalabhasana:
- They are the best yogaasanas for strengthening the muscles of the back
- Gives flexibility to back muscles and spine
- Strengthen shoulder and neck muscles
Those who have severe back problems should do these asanas under supervision of a Yoga instructor
They should be avoided in pregnancy and after recent abdominal surgery
Bhujangasana (The Cobra Pose):
Videos for Bhujangasana:
How to do?
- Lie down on your stomach with the hands on the side, toes touching together
- Bring your hands to the front at the shoulder level, with palms resting on the floor
- Slowly raise your trunk and head with the support of the palms alone. The arms should be bent at the elbows
- Arch your neck slightly backwards so that the pose looks like a cobra with a raised hood
- Breathe normally and feel the stomach press against the floor.
- Hold the asanas for few seconds in the beginning stages
- You can do up to 2 minutes at a stretch with practise
- You can release the pose by bringing the hands back to the sides and resting your head on the forehead
- Then, place the hands under your head like a pillow
- Bend and rest your head on one side and breathe normally
Benefits of Bhujangasana:
- It strengthens the back muscles especially those of the lower back
- It increases the flexibility of the spine and the muscles around it
- It tones the organs of the lower abdomen, the digestive organs, the urinary organs and reproductive organs
Note:
Don’t do this exercise if you are a pregnant or if you have undergone any abdominal surgeries recently

Weightless squats:
Repeated weightless squats either reduces or relieves pain
You should go from your squatting position to standing position repeatedly
How to do?
Try this combination / circuit:
- 15 push ups
- 30 weightless squats
- 400 meter jog
Repeat the above circuit as many times as possible in 15 minutes time.
Benefits:
- They will build up muscular strength and help with your balance
- Stretches some muscles which are tight
Back Arch:
This is also an important stretching exercise for back pain which also heals pain in the coccyx and sacrum area
How to Do?
Step 1:
- Stand with your feet about shoulder width apart
- Your toes should point outwards
- Rest your hands on your thighs just above your knees with your fingers and thumb facing inwards
- Take a slow deep breath through your nose
- Exhale through your mouth as you slowly and gently bend your head down towards your chest and push your hips and pelvis forwards
- Feel your entire spine stretching from your neck to your back and sacrum.
- Stretch as far as you comfortably can and until you have fully exhaled. This should take about 4-5 seconds. Pause for a second or two.
Step 2:
- Breathe in through your nose as you slowly and smoothly raise your head up.
- Continue until you are looking above and behind your body.
- At the same time, tilt your hips and pelvis back so that your backside is sticking up in the air
- Arch your spine as far as you comfortably can
- Hold the position for a couple of minutes
Step 3:
- Exhale through your mouth as you slowly and gently lower your head and your backside into the back stretching position in step 1, i.e. with your head resting near your chest and your hips and pelvis pushed forward
- Continue to alternately stretch and arch your back 5 to 10 times to begin with
- Build up to 15-20 times in a session or simply do it for a few minutes at a time
Benefits:
- Limbers and stretches your back and neck muscles
- Stimulates your spinal nerves
- Aligns your vertebrae
- Promotes blood flow
- Relieves back, neck, sacral and coccyx pain and stiffness
Lumbar and Sacrum Rub:
It is an excellent exercise for low back pain and stiffness. It also strengthens the kidney
The exercise warms and stimulates the muscles in the lower back and sacrum, which enhances blood and energy flow. This has a therapeutic effect on the kidneys and eases and prevents pain and stiffness in this area.
How to do?
It can be done in sitting or standing position
Step 1:
- Stand with your feet parallel, about shoulder width apart
- Transfer all your weight down into your legs
- Alternate: sit on the front edge of a firm chair
- Take of your shirt (or raise it so that your lower back is bare)
Step 2:
- Rub your hands together briskly until they feel hot
- Immediately place them on your lower back on either side of your spine, right hand on the right side and the left hand on the left side
- Rub up and down your lower back and sacrum with fairly firm strokes
- Feel the heat building
- Alternate: Clench loose fists and use the backs of your hand and knuckles to do the rubbing
- Continue for 1-2 minutes. If your hands or arms get sore, briefly stop, but leave your hands on your back to keep the heat in – then continue
- As soon as you finish put your shirt or pull it down to keep the area warm
Benefits:
- Warms and limbers the lower back and sacrum
- Enhances blood and energy circulation in this area
- Strengthens the kidneys
- Relieves and prevents low back pain and stiffness
Note:
- This exercise is an excellent therapy for acute and chronic lower back pain
- It should be done the first thing in the morning and again at the night
- Add some liniment beforehand for greater pain relief
- It can be used as a part of daily exercise routine or pre-sports warm up
The Thigh Burner:
It is one of the best thigh exercises
In conjunction with deep breathing forms, Thigh Burner forms one of the most powerful inner thigh exercises
It strengthens your thighs, knees and pelvic area, tightens your butt
It builds strong, toned thigh and legs
How to do?
Step 1:
- Stand with your feet turned outwards and more than shoulder apart
- Bend your legs and sink your weight down into your thighs so that your thighs are parallel to the ground
- Place your hands on your thighs, with fingers facing inwards
- Keep your spine straight
- Look at the ground a metre (3 feet) or so in front of you
Step 2:
- As you hold the above position, commence slow deep breathing through your nose.
- To enhance the effects, as you exhale tighten your butt muscles and your abs.
- Relax as you inhale
- Try to hold this position for 30-60 seconds
- Feel your inner thigh muscles and tendons stretching
- Slowly stand up and take a slow deep breath or two
- Sink back down and repeat the exercise
- Do it a couple of times to begin with
- Build up to 4-5 times in a session
- Alternate: Do just one thigh burner in a session but hold it for as long as you can. Increase the time a little each day.
Benefits:
- Stretches your inner thighs
- Strengthens your thighs and knees
- Tones and tightens your gluteal muscles (butt muscles)
- Strengthens your pelvic area
Note:
- Slow deep breathing during the exercise greatly enhances the benefits
- Contract your butt and ab muscles as you inhale, for extra benefit
Treadmill:
Workout: 4 times a week for 40 minutes + 20 minutes jogging + 20 minutes fast walking
Hamstring stretch:
How to do?
- Put one foot forward and Extend one leg backwards with the foot flat on the floor and not bending the knee.
- Lean gently forward bending the front leg, don’t strain the rear leg
- Leaning can be done against the wall, on the kitchen work surface scanning the newspaper headlines or on the back of the chair looking at the TV
Benefits:
Relaxes the tight back and hamstrings
Inversion therapy:
How to do?
- This involves hanging upside down at an angle on an inversion table with the feet fastened in position
- This applies traction to the spine
Breathing and Relaxation exercises:
Breathing and relaxation exercises when combined with deep tissue massage give good pain relief in coccydynia. Rolfing is a technique of deep tissue massage and is usually performed over 10 sessions. Rolfer’s work on major muscle groups, especially the pelvis. They focus on all muscles but they focus on all muscles of your pelvis, low back, butt and upper legs
Yoga:
Beneficial Yoga exercises which can soothe your coccyx pain are:
Kegel exercises or pelvic floor exercises are one of the effective ways of dealing with coccydynia.
It is specially indicated for women who have just given birth (during pregnancy and delivery process, the coccyx has a huge tendency to get overstretched)
Kegel exercise is helpful in controlling the pain and also strengthens the pelvic floor.
How to do it?
- This exercise may be performed by controlling the flow of urine
- When you do so, you are contracting the pelvic floor muscle and at the same time strengthening it
- It is suggested that you perform this without having to squeeze the gluteus muscle and as well as the thighs
Cat / Cow Stretch:
How to do?
- Place the body in a prone (faced down) table-top position with the hands directly under the shoulders and the knees directly under the hips
- Round your back up to the sky (cat) and then arch your back with your head lifting up (cow).
- As a cat stretch is performed, exhale
- As the cow stretch is performed, inhale
- Perform this exercise for 1 minute
Benefits:
- Limbers and stretches the back and neck muscles
- Stimulates the spinal nerves
- Aligns the vertebrae
- Promote blood flow
- Relieves back and neck pain
Spinal Twist:
How to do?
- Lie down on your back
- Bring the left knee into your chest
- The right leg is extended on the floor
- Lower your left knee across the right leg
- For an added stretch, place your right hand on your left knee, gently pressing it downward
- Look over your left shoulder
- Keep your shoulders in contact with the floor
- Hold stretch for 1 minute
Benefits:
- It releases the lower back
- Stimulates blood flow to the internal organs and spine
Understanding the disease
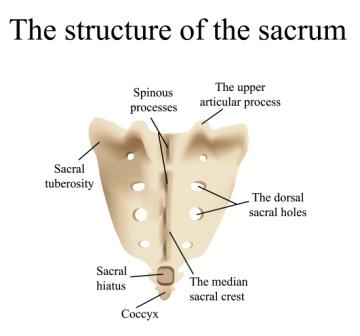
Anatomy of Coccyx:
- The coccyx or tailbone is the very bottom portion of the spine. It is a small triangular bone at the base of the spinal column (backbone). It is located just above the cleft in the buttocks and curves forwards so that it points towards the front of the body. It represents a vestigial tail or the tail bone. It consists of 3-5 very small bones fused together. Movement between the bones is permitted by the fibrous joints and ligaments.
- Derivation – The word coccyx is derived from the Greek word for cuckoo. It resembles the beak of a cuckoo.
- Articulations: The coccyx articulates with the sacrum through a vestigial disc and is also connected to the sacrum with ligaments. There is very limited movement between the coccyx and the sacrum. The attachment is either a symphysis (Fibrocartilaginous fusion between 2 bones) or is a true synovial joint.
- Ventral side: (part facing front) – This part is slightly concave and dorsal side is convex.
- Transverse grooves: Present on both ventral and dorsal sides. These grooves show where the vestigial coccyx units had fused previously
- The coccyx bones become more flexible in pregnant women to facilitate them to give birth more easily
- Coccyx bears the weight of our body when we sit down.
- Muscles inserting on the anterior coccyx include the levator ani, which is sometimes considered as several separate muscle parts including the coccygeus, iliococcygeus and pubococcygeus muscles. This important muscle group supports the pelvic floor (preventing inferior sagging of the intrapelvic contents) and plays a role in maintaining faecal continence. Muscles originating on the posterior coccyx include Gluteus maximus, which is the largest of the gluteal muscle (buttock muscle) and functions to extend the thigh during ambulation.
Function of coccyx:
- Coccyx serves as a weight-bearing structure when a person is seated, thus completing the tripod of weight bearing composed of the coccyx and the bilateral ischium.
- The coccyx bears more weight when the seated person is leaning backward. Therefore many patients with coccydynia sit leaning forward which shifts more of the weight to the bilateral ischium rather than coccyx. Alternatively, patients with coccydynia may sit toward one side so that the body weight is exerted mainly on the ischial tuberosity with less pressure on coccyx. Such side leaning may lead to concomitant ischial bursitis in addition to the antecedent coccydynia.
Synonyms, orientation
Coccygodynia, Coccygeal pain, Coccyx pain, Coccalgia
Orientations of the Coccyx: (As described by Postacchini and Massobrio)
- Type I orientation – Coccyx is curved anteriorly (towards front) with its apex (tip) facing downward and caudally
- Type II – Forward curvature is more and the apex extends forward
- Type III – Coccyx angles forward sharply
- Type IV – Coccyx is subluxated at the sacro-coccygeal joint
Note: Subluxation – Partial dislocation / displacement / malalignment
Causes
Coccyx pain is caused if an injury or pressure on the area causes the bones to move beyond their normal range (very limited) of motion. This results in inflammation and pain. An injury to the vestigial disc or the ligaments in the coccygeal area may also cause pain. Rarely fracture of the bones of the coccyx, tumour or infection in the coccyx can also cause pain.
Coccygodynia can occur when something damages the coccyx or its surrounding areas such as:
- Muscles and ligaments supporting the coccyx getting stretched out of place as is caused during childbirth
- Trauma to the coccyx caused due to an accident
- Pulling the coccyx out of its normal position, either through poor posture or repeated activity such as cycling or rowing
The below mentioned are the causes for Coccygeal pain
- Idiopathic Coccydynia: Wherein the cause is unknown. At least 1/3 of all those who suffer from coccydynia belong to this category. It has been described in the absence of any obvious pathological changes involving the coccyx. In these patients, the pain may actually result from spasticity or other abnormalities affecting the muscles of the pelvic floor.
- Injury / Trauma – Injury is probably the main common cause of coccydynia but it seems to be spontaneous. A fall on the tailbone causes inflammation or injury to the coccyx or coccygeal attachment of the sacrum.
Acute abrupt trauma includes –
Internal trauma – Ex. Childbirth
External trauma – Ex. Falling onto the coccyx
Non-abrupt trauma –Prolonged sitting
The trauma to coccyx can occur in –
Following a fall
Horseback riding
cycling and skate boarding injuries
Childbirth – During childbirth, the head of the baby passes over the top of the coccyx. The pressure created against the coccyx can result in injury to the coccyx structures (the disc, ligaments, bones). The pressure can also cause fracture of coccyx (not common).
Pressure – Certain activities that put prolonged pressure on the tailbone.
Examples –
Persistent pressure from activities like bicycling
Increased sitting
Sitting improperly
Sitting on hard surface for long periods of time
Horse riding
The pain caused by these is usually not of permanent nature. If the inflammation and symptoms are not managed, the pain may become chronic.
- Primary or metastatic malignancies (Tumours): Presence of sacrococcygeal teratoma or other tumours around coccyx (Surgery and chemotherapy are the options)
- Infection to coccyx and related structures
- Abnormal / Excessive mobility of the tailbone
- Fractures and dislocations of coccyx bone
- Age related ‘wear and tear’ of the bone and soft tissues may contribute
- After certain medical procedures like colonoscopy
- Tumour or infection: Tumour or infection in the coccyx area puts pressure on the coccyx causing coccydynia (rare)
- Pathological instability:
Most cases of Coccygeal pain occur either due to a subluxated coccyx or hyper-mobile coccyx. This pathological instability may give rise to chronic inflammatory changes.
Many patients report a history of an antecedent traumatic event, which has been shown to be associated with coccygeal instability, particularly posterior subluxation.
Body Mass Index (BMI) and Obesity:
BMI influences the prevalence of coccydynia.
Obesity is 3 times more common in patients with tailbone pain than in normal population. This shows that obese and over-weight patients have more risk of getting coccydynia in comparison to the normal lot.
Note: Coccydynia due to the above said causes (other than tumours) is not permanent. If not controlled, it may become very persistent and chronic.
Other ways in which Coccyx pain develops:
- Partial dislocation of the sacrococcygeal synchondrosis that can possibly result in abnormal movement of the coccyx from excessive sitting
- Repetitive trauma of the surrounding ligaments and muscles resulting in inflammation of the tissues and pain
Epidemiology / Prevalence
- Coccydynia is considered to be rare. It accounts for less than 1 % of back pains reported by the physicians
- Women are affected more frequently than men. The ratio is 5:1.
- It can occur in children and adults
- Degenerative changes of the sacro-coccygeal junction and the intra-coccygeal junctions as well as fusion at these sites seem to increase with age.
- Although it may affect individuals of all ages and of either gender, the mean age of onset has been shown to be 40 years and the prevalence is 5 times greater in women than in men.
- No association with ethnicity or race.
Why do more coccyx injuries occur in women than in men?
- The women’s coccyx is rotated, leaving it more exposed to injury
- Women have a broader pelvis, which means that sitting places pressure on their coccyx (male anatomy causes them to sit without much pressure on the coccyx)
- Childbirth is a common cause of Coccydynia
Important points about coccyx pain
- Patients with coccydynia often present with complaints of pain in and around the coccyx without significant low back pain or pain radiation or referral.
- Incidence of concomitant low back pain is known to be higher in individuals with coccydynia in comparison to the general population. This is particularly found in people with certain anatomic variants such as a coccyx that is curved forward with an apex pointed caudally or straightforward.
- Classically the pain is associated with sitting and is exacerbated when rising from a seated position
- Many people will feel a frequent need to defecate or pain with defecation
- Some may report pain relief when they sit on their legs or one buttock
Diagnosis
It should be first determined if the pain is related to coccyx or due to non-coccygeal causes because lower back pain or pain while sitting can occur due to number of other causes.
The below mentioned investigations rule out various causes which are not related to coccyx –
- Physical / rectal examination
- High resolution X-rays
- MRI scans
The causes not involving coccyx are:
- Tarlov cysts
- Pain referred from higher up the spine, such as problems in uterus, intestines, radiating to lower back region.
Fractured coccyx – In this, the coccyx is dislocated at an intercoccygeal joint
Physical examination:
A thorough physical examination for coccyx pain should include:
Pelvic and rectal examination to check for a mass or tumour that could be a cause of the pain
Palpation to check for local tenderness
The most striking finding on examination is usually the local tenderness upon palpation of the coccyx.
If the coccyx is not tender to palpation then the pain is referred from another structure such as a lumbo-sacral disc herniation or degenerative disc disease
Pelvic examination: Soft tissues overlying the sacro-coccygeal region should be inspected for the presence of pilonidal cysts (they represent potentially painful in-growths of one or more hair follicles). Palpation of this region reveals localized tenderness and swelling.
A mass like a bony spicule or tumour can be palpated
Rectal manipulation – Manipulation of coccygeal segments or sacrococcygeal joint by rectal manipulation will elicit pain
Test for coccygeal pain
- A local anaesthesia is injected into the coccygeal area. If the pain is related to the coccyx, it reduces and there is immediate relief.
- If this anaesthetic test is positive then a dynamic (sit/stand) X-ray or MRI scan show whether the coccyx dislocates when the patient sits
Other investigations:
- Stool guaiac test should be done for occult test to assess for Gastro-intestinal pathology
- Dynamic radiographs obtained in both sitting and standing positions may be more useful than static X-rays because they allow for measurement of the saggital rotation of the pelvis and the coccygeal angle of incidence. A comparison of sitting and standing films will yield radiographic abnormalities in up to 70% of symptomatic coccydynia
- MRI and technetium Tc-99m bone scans may demonstrate inflammation of sacrococcygeal area indicative of coccygeal hypermobility
- Provocative testing of the coccyx such as pressing on the region with a blunted needle to elicit pain and pain relief with injection of local anaesthesia under fluoroscopic guidance may be helpful in diagnosis
- Basically the diagnosis of coccydynia is done by a health care professional by taking a thorough medical history from the patient and completing a physical examination
- X-ray of the sacrum and coccyx – to rule out an obvious fracture or a large tumour
- An MRI scan to rule out infection or spinal tumour as a cause of pain
- Bone scans and CT scans give little information. They are generally not done. Typically all imaging studies will be negative.
- A thorough inspection / palpation of this area is needed to detect any abnormal masses or abscesses (infections)
- A lateral X-ray of the coccyx is taken to help detect any significant coccygeal pathology such as a fracture
Differential Diagnosis
Coccyx Fracture (broken tailbone):
It presents with –
- Pain that increases in severity when sitting or getting up from a chair or when experiencing a bowel movement
- Provoked pain over the tailbone
- Nausea
- Bruising or swelling in the tailbone area
Sacro-coccygeal dislocation:
- It is a rare injury
- Presents with pain in the sacro-coccygeal area generally followed by a fall or injury
- On examination, a step will be felt in the continuity of sacrum and coccyx
- The tip of the coccyx will not be palpable
- Per rectal examination reveals a small bump on running the finger along the sacrococcygeal curvature
- Plain radiographs of sacrococcygeal region – reveals anterior dislocation of coccyx over sacrum
Intracoccygeal dislocation: Here there is dislocation of one coccygeal segment from the other
Intrapelvic malignancy and / or metastatic lesions
Ischial bursitis / Ischiogluteal bursitis
- Ischial bursa (small sac filled with lubricating fluid) is located in the upper buttock area
- Inflammation in this bursa is called Ischial bursitis
- It causes dull pain in this area which is most noticeable when climbing uphill
- The pain sometimes occurs after prolonged sitting on hard surfaces
- It is also called as ‘weaver’s bottom’ or ‘tailor’s bottom’
Sacro-iliac joint pain or Sacroiliac joint dysfunction:
- It presents with pain in sacroiliac joint
- Pain is experienced often in the lower back or at the back of the hips
- Pain is sometimes present in the groins and thighs
- Pain is typically worse with standing and walking and improves while lying down
- Stiffness and burning sensation can be felt in the pelvis
Ovarian cyst:
Most ovarian cysts are never noticed and resolve before being tracked or coming to a woman’s knowledge about its presence.
Most common symptoms caused by a cyst are:
- Abdominal pain
- Pelvic pain
Pain may be due to:
- Rupture of the cyst
- Rapid growth and stretching
- Bleeding into the cyst
- Twisting of the cyst around its blood supply (torsion)
Large cyst can produce the below said symptoms as a result of pressure or distortion of adjacent anatomical structures:
- Fullness (bloating)
- Indigestion
- Early satiety (feeling full after eating small amount of food)
- Urinary urgency
- Feeling an urge to defecate
- Difficult bowel movements
- Pain with sexual intercourse
- Low back pain
Uterine fibroids:
Uterine fibroids are very common non-cancerous (benign) growths that develop in the muscular wall of the uterus. They can range in a size from very tiny to larger than a cantaloupe. Occasionally, they can cause the uterus to grow to the size of a 5 month pregnancy
Symptoms are mild to none in many women.
Most common symptoms in symptomatic fibroids are:
- Heavy menstrual bleeding that can cause anaemia
- Bleeding between periods
- Spotting before or after periods
- Pain – abdomen, pelvis or low back
- Urinary incontinence
- Kidney and ureter blockage (rare)
- Difficulty or pain with bowel movements
- Infertility
- Miscarriage
- Premature labour etc
Pilonidal cyst:
It occurs at the bottom of the tailbone and can become infected and filled with pus (pilonidal abscess)
It presents with the below said symptoms:
- Pain and / or swelling at the bottom of the spine
- Redness at the bottom of the spine
- Draining pus
- Fever
Sacral insufficiency fracture:
- These fractures usually develop in the elderly patients with osteoporosis without definite trauma history.
- It is a common cause of low back pain and is missed in the diagnosis because it presents with signs and symptoms which are similar to several lower lumbar degenerative diseases and spinal trauma
- Possibility of SIF can be suspected in patients who are at the risk of osteoporosis, presenting with sudden sacropelvic pain and tenderness with no or trivial trauma
Endometriosis:
It is a condition in which normal endometrial mucosa is abnormally implanted in locations other than uterine cavity. Approximately 30-40% women with endometriosis will be sub fertile.
Endometriosis presents with:
Dysmenorrhoea, Heavy or irregular bleeding, Pelvic pain, Lower abdominal pain, Low back pain, Dyspareunia, Dyschezia (pain on defecation), Bloating, nausea, vomiting, Inguinal pain, Pain on micturation / urinary frequency and Pain during exercise
Haemorrhoids:
They are swollen blood vessels in the lower rectum (piles).
The symptoms depend on whether the haemorrhoids are internal or external
Common symptoms:
Bleeding per anus, Prolapsed pile mass, Itching and irritation in the perianal area, Perianal pain. Read more about Ayurvedic treatment and tips for hemorrhoids
Lumbar Degenerative Disc Disease: It is one of the common causes for low back pain
Lumbar Facet Arthropathy:
- It is one of the common sources of low back pain (chronic)
Lumbar spondylolysis and Spondylolisthesis
- Lumbar spondylolysis is a unilateral or bilateral defect of the pars interarticularis that affects one or more of the lumbar vertebrae.
- In Greek, spondylolysis means break or defect in the vertebrae
- Spondylolisthesis on the other hand means moving or slipping forward of one vertebra over the next caudal vertebra
- These 2 conditions are the common causes for low back pain
Mechanical Low Back Pain:
- It is the 2nd most common symptom related reason for seeing a doctor in United States. Of the US population, 85% suffer from this condition at some point of their lifetime.
- It presents with low back pain
Piriformis syndrome:
- It is usually caused by the neuritis of proximal sciatic nerve. It mimics diskogenic sciatica
- It is also called pseudo-sciatica, wallet sciatica and hip socket neuropathy
- It presents with buttock pain
Proctalgia fugax:
- It is a variant of levator ani syndrome
- It presents with severe episodic, rectal and sacrococcygeal pain
- It can be caused by cramp of levator ani muscle particularly in the pubococcygeus
Sciatica:
It is a painful condition caused due to irritation, impingement or entrapment of Sciatic nerve in the lower back region
Sciatica presents with pain and tingling sensation in:
- Low back
- Hip
- Buttock
- Thigh
- Outer side of the leg
Infection (including shingles of the buttocks) –
- Shingles is a painful skin rash caused by varicella zoster virus. It is also called as herpes zoster.
- Shingles can occur in the buttock area giving severe pain
Sacroiliitis
- It is the condition of inflammation of sacroiliac joints
- It presents with pain in the sacroiliac joint
- The pain may be referred to lumbococcygeal area, legs and buttock
Referred pain from
- Sacroiliac joint
- Lumbosacral area
- Uterus
- Ovary
- Perirectal abscess
Risk Factors:
- Major risk factor – Injury to the coccyx or pelvic bones
- Ageing – Degenerative changes of the sacrococcygeal junction and the intracoccygeal junctions as well as the fusion at these sites seem to increase with age
- Gender specific risk factor – Trauma related to giving childbirth (Gender specific risk factor). When the baby descends through the mother’s pelvis during child birth it creates substantial pressure on the tail bone causing coccydynia
- Carrying heavy weights
- Sitting while carrying heavy weights
- Sitting on a hard surface
- Obese and overweight people
- Contact sports like basketball, football, hockey etc where there is more chances to fall and not using safety equipment in these sports
Is it possible to prevent coccydynia?
- Coccydynia is associated with injury. Therefore avoiding trauma to the coccyx bone is the best method of preventing coccydynia.
Prevention:
- Body positioning and alignment so as to produce less stress in the coccyx region, correcting daily activities like sitting etc that contribute to pain
- Avoiding bad postures during daily activities
- Not carrying excessive weights can reduce tension and pressure on the coccyx. We should also avoid sitting while carrying heavy weights
- Maintaining body weight also reduces tension and pressure on the coccyx because over body weight and obesity are risk factors for Coccydynia
- Avoidance of contact sports like basketball, football or hockey to reduce chances of falling
- Use of proper safety equipment to prevent coccyx pain. Example – Hockey pants provide extra cushion that protect the thigh, coccyx and buttock. These will help in less falls which will reduce damage to coccyx
- Stretches and strengthening exercises
Coccydynia treatments
A combined approach of:
- Treatments to reduce pain and
- Activity modification to keep the pressure off the tailbone
This approach often controls or alleviates the pain
Non invasive treatments
Non-invasive / Non-surgical method of treatment:
Treatments of coccydynia are usually non-invasive and local. The first line of treatment typically includes:
- Rest
- Avoiding re-injury to the affected area
- Anti-inflammatory medications: Non-steroidal anti-inflammatory drugs (NSAID’s). Common NSAID’s used are ibuprofen, naproxen, COX-2 inhibitors – they help to reduce inflammation around the coccyx which is causing the pain
- Pain medications
- Other pain killers: Tramadol (strong painkiller) – may be required in chronic and severe coccydynia. It may cause side effects like constipation, headaches and dizziness. It is usually prescribed for a short time because it is habit forming (addictive).
- Local cortisone injection (persistent coccydynia) – can potentially relieve pain and even resolve the symptoms for many
- Ice or cold pack to the area several times a day (first few days)
- Avoid sitting for prolonged periods or placing pressure on the area as much as possible
- Use a custom pillow to help take pressure off the coccyx when sitting. For some, a donut-shaped pillow works. Many prefer foam pillow that is more of a U or V shape (with the back open so that nothing touches the coccyx). In short, any pillow or sitting arrangement that keeps the pressure off the coccyx is welcome. A cushion with a cut-out at the back, under the coccyx is recommended while sitting
- If the tailbone pain is caused or increased with bowel movements or constipation, then stool softeners and increased fibre and water intake is recommended
- Physical therapy with exercises can be helpful with recovery
- Increased fibres, stool softeners and mild laxatives are advised if the tailbone pain persists with bowel movements
- Anti-depressants such as Elavil (amitriptyline) – relieves constant pain
- Nerve block injection at the ganglion
- If the pain is due to mal-alignment of the coccyx, manipulation by a chiropractor, osteopathic physician or physical therapist can offer relief
Additional non-surgical treatments (when the pain is persistent or severe):
- Injection: A local injection of a numbing agent like lidocaine and steroid (to decrease the inflammation) provides relief. These are done under fluoroscopic guidance. Relief lasts from 1 week to several years. More than 3 injections per year are not recommended
- Manipulation: Manual manipulation Ex. Chiropractic treatment
- Stretching: It involves gentle stretching of ligaments attached to the coccyx. A physical therapist, chiropractor, physiatrist or other trained healthcare practitioner can provide instruction on the appropriate stretches
- Ultrasound: Physical therapy with ultrasound relieves pain
Note:
Prolonged non-surgical treatment for pain relief and activity modification is a reasonable option provided that the infection and tumour has been ruled out as a cause of pain (through exam, X-ray and MRI scan)
Injections:
They are preferred when oral painkillers doesn’t relieve pain. Below said are the types of injections:
Corticosteroid injections:
- They reduce inflammation (swelling) and pain. They are sometimes combined with local anaesthetic for better efficacy. The pain relief from these may last for several weeks.
These injections cannot cure the condition and too many injections can damage the coccyx and lower back. Thus corticosteroid injections can be taken once or twice a year.
Ganglion impar nerve block:
- Ganglion impar are a cluster of nerves next to the coccyx. It is through these nerves that many of the pain signals travel. A ganglion nerve block temporarily suppresses these nerves by injecting them with a local anaesthesia to stop them transmitting pain signals.
- This can be permanent in a few people while in others the pain will return after a few weeks or months. But the level of pain is usually lower. It is usually safe to have repeated injections of local anaesthesia.
Sacrococcygeal joint injections:
- When these joints are causing coccydynia, the joints are directly injected with a combination of corticosteroids and local anaesthetic.
Spinal manipulation:
- Physiotherapy – In this form of treatment physical methods like massage and manipulation are used to promote healing
- Osteopathy – It is a manipulation technique that can detect and treat problems related to the muscles, nerves and joints
- Chiropractic – It is a manipulation technique based on the theory that many health problems are related to the misalignments of the spine. It helps dealing with these misalignments.
Depression and anxiety which might be present especially if the pain has been there for a long period of time should be treated simultaneously.
Surgical treatment
Surgery should be done when –
- Patients present with cancer (malignancy)
- The tailbone pain has failed to respond to nonsurgical treatment such as medicines, seat cushions and local injections
- Coccygectomy (surgical removal of coccyx) is required in rare cases
Surgery is rarely recommended. Coccygectomy (removal of coccyx) will be considered if the pain is severe and if several months of non-surgical treatment and activity modification have not been effective in relieving the pain
Surgical resection of the coccyx to remove the irritated bone prominence – in presence of unrelenting pain
Surgical approach:
Some doctors prefer removing only a part of coccyx while others recommend removing the entire coccyx.
The operation takes about 30 minutes and can be done on an outpatient basis
It takes a long time for the patient to heal. Generally it takes 3 months to a year after surgery before patients see any relief from their symptoms. Sitting is very difficult throughout the healing process.
Success Rate of surgery:
The reliability and success of the operation depends on 2 main factors –
- Pre-operative patient selection
- Experience of the surgeon, with an experienced surgeon operating on the patients who are good candidates for the surgery
If both the above criteria are fulfilled, then the success rate of 80-90% can be expected from the surgery.
Risks and Complications of the Surgery:
- Injury and infection of the rectum (part of large intestine) which lies in front of the coccyx (happens when the surgeon accidentally moves out of the sub-periosteal plane around the bone during dissection)
- Wound healing difficulties and or local infection
- Continued pain in the coccyx post-operatively (patient has to endure the long healing process and still has not had improvement in the symptoms)
When to look for a doctor (seeking medical advice)?
Take doctor’s help or seek a medical attention if:
- If the pain becomes severe and persistently troublesome
- If there is associated bruising or rash with pain
Some people may be allergic to NSAID’s or have increased risk of developing stomach ulcers. In such cases, painkillers like Paracetamol can be used
Prognosis for Coccydynia
- Many recover completely with the help of conservative treatments or by natural recovery over a period of time. Others develop a persistent chronic pain syndrome at the coccyx area.
- Coccyx pain seems to be more chronic than any other injury sites because of the inability to immobilize or brace the site. This will therefore contribute to delayed or prolonged recovery and also to the development of chronic, persistent, intractable pain syndromes.
- When the coccyx pain becomes chronic (persisting for more than 3-6 months), the chances of it responding to natural recovery or conventional methods of treatment or medication becomes less. The condition will progress indefinitely. It will further become resistant to treatment. Thereafter it will require a multimodal treatment approach (ex. Oral medications with local injections)
- Early interventions like oral medications, injections and physical therapy are presumed to decrease the chance of acute coccydynia progressing into chronic coccydynia. Therefore an aggressive non-surgical treatment early on in the disease is recommended to potentially decrease the chances of lifelong pain and disability.
- Coccydynia is not associated with increased mortality but is associated with substantial morbidity. Patients often report severe and persistent pain which disturbs their functional activities requiring sitting, on a daily basis. It also diminishes the quality of life of a patient.
Research
- Physicians dealing with Coccydynia, specializing in Physical medicine and rehabilitation at New Jersey Medical School have published that – A single local nerve block injection at the ganglion can give 100% relief in coccydynia when it is performed under fluoroscopic guidance
- Study: Only a traumatic event occurring within 1 month of onset is significant in increasing the risk of instability and subsequent coccydynia (Maigne et al.). they showed that the proportion of patients who develop instability following a traumatic event before 1 month of onset is nearly equal to the proportion of people who develop instability without a history of trauma (55% and 53% respectively). The instability rate in contrast was found to be 77.1% when the traumatic event was less than a month previously.
- The coccygeal lesion pattern in different people:
Obese patients – Posterior subluxation
Normal weight patients – hyper-mobility or radiographically normal coccyges
Thin patients – Anterior subluxation and spicules
Coccydynia may be observed in subjects with radiographically normal coccygeal motion. In these cases the symptoms may arise from tumour, infection, bursitis of the coccygeal adventitia, post-traumatic arthritis of sacrococcygeal joint
- Levator ani massage, Levator ani stretching and Sacrococygeal joint mobilization are effective initial modalities for addressing coccydynia (Maigne and Chattelier)
- Wray et al. recommended administering a steroid (40mg methylprednisolone) and long acting anaesthetic (10ml of 0.25% bupivicane) for coccydynia. For patients with persistent symptoms, a 3rd injection was performed in conjunction with coccygeal manipulation.
Coccygeal manipulation: The manipulation was done with the patient in the left lateral position, using eh index finger per rectum and the thumb overlying the coccyx. The coccyx was repeatedly flexed and extended for approximately 1 minute. The combination of injection and coccygeal manipulation provided a success rate of 85%
- Forgel et al. proposed the following therapeutic protocol for acute coccydynia (pain less than 2 months). The first line of treatment should include at least 8 weeks of rest, stool softeners, adjustments in sitting position and NSAID’s.
Ayurvedic Approach of Coccydynia
We cannot find an exact terminology or a disease condition from the texts of Ayurveda which fits into a close comparison with Coccydynia.
The terms Katishula, Trikavedana, Trikashula etc give a closer meaning in relation to Coccydynia. Katishula precisely means back pain or low back pain and Trikashula or Trikavedana means pain in the Sacral, Coccygeal, Sacro-coccygeal and / or Sacro-iliac pain.
Gudagata Vata
The clinical picture of a condition called Gudagata Vata explained in the context of Vata Vyadhi Chikitsa (Treatment of diseases caused due to morbid Vata) closely resembles Coccydynia or tail bone pain.
The term Gudagata Vata means morbid Vata afflicting Guda (anal, buttock or sacro-coccygeal area). The vitiated Vata is said to lodge in the anal region which also encapsulates the buttock and sacro-coccygeal area (lower back) and cause a painful condition called Gudagata Vata
About Gudagata Vata it is said:
The vitiated Vata on getting lodged in the Guda afflicts the structures in that area and causes:
- Vitgraha – Constipation / Disturbed bowel movements
- Mutragraha – Obstruction to urination
- Vatagraha – Obstruction to the passage of flatus
- Shula – Pain abdomen / Colic
- Adhmana – Bloating or feeling of heaviness
- Ashma – Stones in the urinary tract
- Sharkara – gravel in the urinary tract
Vedana (Pain) and Shosha (degeneration) in:
- Jangha – Legs
- Uru – Thighs
- Trika – Sacro-coccygeal region
- Prushta – Back
- Pada – Foot
Actually Gudagata Vata looks like a syndrome with pathological manifestations all over the lower parts of the body viz Large intestine, Urinary Bladder, Kidney, Ureter, Abdominal viscera, Lower limbs and the joints of the spine especially the lower part of the spine.
Looking at this condition in one way it looks like all are related and neighbouring structures.
If we look at the pathology of the disease from the Coccyx pain point of view, Gudagata Vata covers a vast differential diagnosis of the painful conditions occurring in the low back region.
The cause’s contributory to the vitiation of Vata can be taken into consideration as the aetiology of Gudagata Vata with special reference to Coccydynia. Abhighata or trauma is one of the chief causes for Vata vitiation, be it local or systemic. Trauma is also the chief cause and risk factor for Coccydynia.
Prishta shula (back pain), Kati shula / graham (pain or stiffness in the sacral and coccygeal region / Lumbosacral region) and Spik Shula (Buttock Pain) are the terms used in the context of Asthapyaha (patient’s eligible to undergo treatment with decoction enemas) in Charaka Siddhi Sthana chapter 2.
This means to tell that all those who are suffering from Prishta shula, Kati shula and Spik shula can be administered with Asthapana Vasti (and Anuvasana Vasti – medicated oil enema) which is a treatment of choice in Vata disorders with special reference to Rheumatological, Neurological, Neuro-muscular and Musculo-skeletal disorders (Vasti or enema treatment is said to be half of all the other treatments put together, thus the scope of administration of Vasti is large and can be used in wide array of psycho-somatic illnesses)
Ayurvedic Treatment options
All treatments predominantly addressing the morbid Vata shall be used in the treatment of Coccydynia. The associated Dosha’s (Pitta or Kapha) if any should be tracked down by the Ayurvedic physician while conducting a thorough clinical examination and treated accordingly. The tissue strength especially that of bone, bone marrow, muscles, flesh and fat should be analysed.
The prakriti (constitution of the patient) and vikriti (morbidity, its quality, quantity and strength) should be thoroughly analyzed after having done with Roga (disease) and Rogi (diseased) Pareeksha (examination). This will help in making accurate choice with respect to the treatment, diet and medicines to be prescribed.
The best Ayurvedic treatment options for Coccydynia are as said below:
Sthanika: (Local treatment)
Abhyanga – Massage with medicated / herbal oils
Care should be taken to analyze the extent of pain and injury before sorting out to Abhyanga. Vigorous massage should anyhow be avoided.
Kati Vasti – Oil pooling in the low back area extended so as to cover the coccygeal part
Avagaha: Tub bath or Sitz bath by making the patient to sit in the tub filled with medicated oil. Milk processed with Dashamula (group of 10 herbal roots) and Laksha (LAC) can be used for Avagaha
The below mentioned oils shall be used for Abhyanga, Kati Vasti, Avagaha:
- Murivenna – a renowned oil for non healing wounds, fractures and sprains.
- Ashwagandhabala Lakshadi Tailam
- Ksheerabala Tailam
- Mahanarayana Tailam
- Dhanwantara Tailam
- Sahacharadi Tailam
- Mahamasha Tailam
- Pinda Tailam etc
Pinda sweda: Medicated bolus fomentation / steaming / sudation
This is usually done following Abhyanga. In combination Abhyanga and Pinda Sweda provide pain relief and improve the movements. They relax the stiff muscles and soft tissues around the coccyx. 2 variants of Pinda Sweda can be tried in Coccydynia.
- Patra Pinda Sweda – Bolus fomentation with medicated leaves like Nirgundi (Vitex negundo), Eranda Patra (Castor – Ricinus communis leaves) etc
- Shashtika Shali Pinda Sweda – Fomentation with Shashtika rice processed in milk prepared with herbal decoctions. This treatment apart from healing property also has nutritive property.
Abhyantara Chikitsa: Internal treatment
Snehapana (Nitya) – Oral consumption of medicated oils / ghee / oils and ghee in daily metered doses is called Snehapana. Snehapana helps in healing the trauma, reduces pain & nourishes the bones, soft tissues and joints.
The medicines used for Snehapana are:
- Guggulutiktaka Ghritam
- Rasnadi Ghritam
- Mahamasha Tailam
Virechana (Nitya) – Herbal purgation is given by administering daily metered doses of medicated oils / ghee. Apart from clearing the bowels, they improve metabolism, enhance blood circulation, soothes nerves, detoxifies the body and controls Vayu which is the chief culprit in causing the pain.
When the bowel and bladder are kept clean and clear, the pressure on the sacrum and coccyx is reduced. Churna (powder) or Leha (confections / jam) can also used for giving purgation but oils are generally preferred for having antagonistic property towards Vayu
The medicines used for this purpose are:
- Gandharvahastadi Eranda Tailam
- Nimbamritadi Eranda Tailam
Vasti: Medicated enemas are said to be the best treatments for controlling Vayu and thus tackling the other morbid factors in the body. Enemas not only help in cleansing in the bowel, they also set right the metabolism, soothe the nerves, flush the toxins, regularize the functions of all the tissues, gets rid of stress, helps recover from the diseases, prevent the recurrence of the diseases and provides immunity. Enemas are specially indicated in bone, joint and soft tissue injuries.
Enemas too can be given in different forms (choice is made on the type of morbidity and strength and constitution of the patient) –
Kashaya Vasti or Asthapana Vasti: Enemas with herbal decoctions
Ksheera Vasti: Enema is given with milk medicated with herbal decoctions. It is a variant of Kashaya Vasti.
Sneha Vasti / Anuvasana Vasti: Enemas with herbal oils, can be used individually or in combination with Kashaya / ksheera vasti.
Matra Vasti: It is a variant of Anuvasana Vasti or Sneha Vasti. This enema is administered on a daily basis for the prescribed duration in small doses.
Some Important Vasti’s which are useful in Coccydynia:
- Erandamuladi Kashaya Vasti
- Dashamula Kashaya Vasti
- Dashamula Ksheera Vasti
- Sneha / Anuvasana / Matra Vasti with Guggulutiktaka Ghritam
Oral Ayurvedic medicines
Best oral medications for Coccydynia:
Kashayam (herbal decoctions)
- Maharasnadi Kashayam
- Dhanwantaram Kashayam
- Gandharvahastadi Kashayam
- Sahacharabaladi Kashayam
Medicated oils and ghee:
- Sahacharadi Tailam
- Guggulutiktaka Ghritam
- Rasnadi Ghritam
Tablets and capsules
- Vata Vidhwamsini Rasa
- Valiya Marma Gulika
- Yogaraja Guggulu
- Lakshadi Guggulu
- Trayodashanga Guggulu
- Ksheerabala Tailam 101 – oil or capsules
- Dhanwantaram 101 – oil or capsules
- Gandha Tailam / Gandha tailam capsules
Bhasma
Interesting facts
Interesting points about Coccydynia:
- Coccyx pain was first documented in 1588 and the term coccygodynia was coined by Simpson in 1859. Currently the term coccydynia is used more.
- In the 1900’s coccydynia was a popular diagnosis for all types of lower back pain. An extreme form of treatment, the surgical removal of the coccyx (coccygectomy) was commonly undertaken to treat the low back pain. This operation had variable results.
- In the later period it was (pain and failure of operation) in some way related to neurosis because coccydynia was mostly common among women. The corollary was ‘if the operation did not work it was because the pain was in the individual’s head’. The operation lost its reputation and was never performed in the later period of time.
- In the present time it is known and believed that coccydynia as a medical condition exists. However it is fairly uncommon.
References
http://emedicine.medscape.com/article/309486-overview
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2682410/
http://www.medicinenet.com/coccydynia/article.htm#coccydynia_facts
http://www.spine-health.com/conditions/lower-back-pain/coccydynia-tailbone-pain
http://www.nhs.uk/Conditions/coccydinia/Pages/Treatment.aspx
https://my.clevelandclinic.org/health/diseases_conditions/hic_Coccydynia_Tailbone_Pain
You have the best remedies in the form of treatments and medicines to relieve you from the pain of Coccydynia in Ayurveda but don’t forget to consult an Expert Ayurveda Doctor for an opinion before starting on with anything
Ayurveda helps you to ‘Sit better & work’
Consult Dr Raghuram by skype or email



4 comments on “Coccydynia, Coccyx Pain – Exercises, Remedies, Natural Tips”
Ismail zabihullah ahmadzai
thanks alot i had a problam of backone whicl is called coccydynia so thanks … i will do excercise …. because excercise is so so usefull than medicene . so thankls alot
Dr Malini Bhat
You are welcome sir.
VJ
Excellent article sir…I too have similar kind of pain and undergoing Ayurvedha treatment (vasti) by an experienced doctor in Hyderabad.However the process is very slow and will take time to become normal.
joemascarenhas
Hi Venkat did you find an improvement after you posted this comment and what exactly did you try as a solution for the pain. Thankyou.